
The Half Cup Problem
A five-hour runner does the math — and discovers what forty-two years of running never told him


Editor's note, May 28, 2026: Manitoba Marathon staff have confirmed a 16th aid station at km 40, operated by community volunteers from a local church. This station will carry XACT in 2026. All tables and references to station count in the Manitoba section have been updated to reflect 16 stations.
I never asked enough questions. I have now. I now have some knowledge. And I am passing it on.
For every runner who has ever crossed a finish line wondering why their legs stopped working — and never thought to ask what was in the cup.
The Promise
The website said it plainly:
That is RunCzech’s own language. Their words. Published on the official Vodafone Prague Marathon 2026 event page, beneath the World Athletics Elite Label badge and above the registration button.
I read it before I flew to Prague.
I believed it.
Why wouldn’t I?
This was the 31st edition of the race. A World Athletics Elite Label event. One of the largest sporting events in the Czech Republic. RunCzech’s own April 28, 2026 press release stated that more than 11,000 runners from more than 100 countries would stand at the start. As of May 27, 2026, the official results page records 9,066 finishers.
I have run nine marathons, multiple half marathons, 10Ks, relays, a half Ironman - a Tinman Triathlon, across three countries over 42 years. I am not an elite runner. I do not pretend to be one.
But I do know what a well run race feels like.
I also now know what it feels like when the system works on paper but not under a five hour runner’s feet.
On race morning, the promise had to become infrastructure.
That is where things began to break.
The Race I Thought I Was Running
I had a plan going in. It was simple.
I expected 16 aid station encounters along the course — 12 physical stations, with 2 pairs each counted twice on the out-and-back sections. My intent was to drink Gatorade at most stations, and plain water at the stations where I took gels, to avoid the gastric emptying problem that arises when concentrated carbohydrate and sports drink are combined in the stomach at marathon pace. Five gels total, spaced roughly every 7 km.
After 42 years of running, my pre-race focus was on carbohydrate. Pasta and white bread in the days before the race. Gels timed to the kilometre markers. Sodium was an afterthought — if I thought about it at all. After all, wouldn’t 11 encounters with Gatorade be more than enough?
Only one slight problem.
The Prague Marathon did not provide electrolyte drink at all 16 encounters.
Electrolyte drink was available at eight of them. Water was available at all 16. RunCzech had published this distinction in advance: refreshment stations (water, Gatorade, fruit, salt, sugar) and refreshing stations (water only), alternating throughout the course. I had not read that distinction carefully enough. I own that mistake.
But what I did not understand until later was how much the distinction mattered for a runner like me.
I was hoping for a four hour finish, though I had conservatively declared 4:30 on my entry form. That put me in Corral K — the eleventh of twelve corrals — alongside roughly a thousand other runners with similar expected pace.
The race started at 8:00 AM.
I ran 5:06.
That gap matters. A four hour runner and a five hour runner are not in the same race. They are not in the same weather. They are not under the same heat load or the same cumulative sodium loss.
The race I had planned for ended at noon. The race I actually ran kept me on course until after 1 PM, well into the warmest part of the day. Race-day conditions began at approximately 7 to 12°C at the start and warmed to approximately 22 to 26°C or higher as the morning progressed (per AccuWeather historical data for Prague, May 3, 2026) — meaning elites finished in cool morning air while back-of-pack runners completed their final kilometres in peak afternoon heat. RunCzech’s own post-race medical article reported conditions reaching 30°C under direct sun on course. (RunCzech, May 13, 2026.) The gap between the official air temperature and the on-course figure reflects what slower runners actually experienced: prolonged exposure under direct sun, long after the shade of the early morning had gone.
The variables shifted under me. I did not adjust — because I did not yet understand what had shifted.
A marathon hydration system should not depend on a tired runner decoding subtle terminology under heat, pace, and fatigue. The 2:30 runner is done before the sun is overhead. The five hour runner is still out there when the course has warmed, volunteers are tired, tables may be strained, and the body has had two or three additional hours to lose water, sodium, carbohydrate, and muscular control.
That is where the model becomes fragile.
Prague may have followed a familiar template. The template itself may be the problem.
What I Saw at 33.5 km
At approximately km 33.5, I encountered the most troubling station of the race.
One volunteer remained under a bridge, pouring water from a bottle into cups for individual runners. One table appeared to remain active. At least two tables appeared to be dismantled or carried away while runners were still arriving. A Komwag municipal services truck — the misting vehicle referenced in RunCzech’s pre-race guide — was deployed further up the road on nábř. E. Beneše, one of the most exposed, shadeless stretches of the entire course. Komwag provides municipal services including street cleaning and groundskeeping; their water supply is not certified as potable. For cooling spray, that is standard practice. For any runner in distress reaching for liquid at km 34 to 36 in 30°C heat, the distinction matters.
I finished 7,681th out of 9,066 finishers. That means at least 1,385 official finishers came in after me — and a substantial number were still behind me when I reached that point.
That matters, because at 33.5 km the station was water only by design. No Gatorade. No fruit. No salt. No sugar. Water only.
Plain water matters. It can help a runner rinse the mouth, swallow a gel, cool the head, wet the neck, lower perceived heat stress, and buy time until the next electrolyte station. But plain water does not replace sodium. A water only station has a different job from an electrolyte station. It is a bridge, not a replacement.
At km 33.5, that distinction became personal.
I stood in line because I needed water for a carbohydrate gel that happened to have sodium in it. The sodium was in my pocket. The race supplied the water that helped me swallow it.
A runner without sodium gels, salt tablets, or carried electrolyte mix reached the same station and found water only.
For me: water plus gel equalled fluid support plus carbohydrate supplementation plus sodium support. For another runner: water plus nothing equalled water.
That is not the same physiological station.
Prague’s water only stations were most useful to runners who had already brought the missing sodium with them. The race did not solve my sodium problem at 33.5 km. My pocket did. After more than four hours on course, that distinction is not academic. It is the difference between an aid station and a partial aid station.
The Finish Line Was Not the Finish
I eventually crossed the finish line.
But the finish line was not the finish.
After the race, I wrote to RunCzech about a number of concerns I had experienced on course — a complaint described more fully later in this piece. In their email reply, RunCzech confirmed that runners were required to walk several hundred metres along Celetná Street before reaching the final refreshment station. My own estimate, walking the route through the controlled finish area and subsequently measuring it, was approximately 460 metres.
Half a kilometre.
I understand the need to maintain safe finisher flow. Runners cannot simply stop under the finish arch. But finisher flow is not a reason to place basic recovery nutrition and hydration half a kilometre from the finish. It is a reason to design a proper recovery chute — one that allows marathoners to keep moving through clearly marked stations containing water, electrolyte replacement, fruit, and carbohydrate replacement, then continue out toward the streets of Prague.
That would preserve flow. It would also ensure that every finisher passes through recovery support before exiting, and allow medical personnel to observe runners for collapse, confusion, heat illness, or dehydration during the critical period immediately after finishing.
As designed, tired runners finishing after four, five, or six hours were expected to walk several hundred metres before reaching basic recovery food. For a runner who has just completed 42.195 km, that distance is not trivial. It is a significant additional demand at precisely the point where recovery support should be most visible and easiest to access.
Many runners I observed appeared to leave the finish area before encountering the final refreshment location. I kept walking because I assumed there had to be something somewhere. Eventually, I found it. A banana. Water. At the far end of the old starting corrals — the place where Groups K and L had stood hours earlier. The back of the pack. Again.
What I Consumed, What I Lost
At the time, I thought I had hydrated reasonably well. I had taken fluid at every station. I had used gels. I had finished. That felt like evidence that the system had worked.
Then I counted.
I consumed one cup of fluid at each of the 16 aid station encounters. When Gatorade was available, I usually took one cup — except at two electrolyte stations where I took plain water with a gel instead. The reason was sound: gel manufacturers commonly recommend water rather than sports drink as the washdown, because combining concentrated carbohydrate with sports drink raises gastric osmolality and can slow emptying. I followed that recommendation, but I did so without realising I was bypassing Gatorade that would not appear again for several kilometres.
Two stations multiplied by approximately 67.5 mg of sodium equals 135 mg of sodium I chose not to take, assuming a 150 ml half cup at a working estimate of 450 mg/L. That lost opportunity is my fault. Runner error and course design failure are not the same category of problem, even when they compound each other. I missed the practical consequence of the alternating station design. I paid 135 mg for the inattention.
But that is not the same as the information RunCzech did not publish.
The station designations were on the website. The product category — Gatorade Isotonic — was disclosed in the racer FAQ. What RunCzech did not publish, to my knowledge, was the delivered concentration on course: whether the drink was supplied as bottled ready-to-drink Gatorade or mixed from powder or concentrate; what dilution protocol was used; how much volunteers were instructed to pour into each cup; and whether late race top-ups preserved the intended concentration.
In other words: what an average cup of Gatorade on course could actually supply in the form of sodium. What the purpose of having Gatorade on course was all about.
Those details are not trivia. They are the numbers that turn a course map into a hydration plan.
Using the 0.3 L cup visible in RunCzech Instagram photography as the best available benchmark, and assuming a practical half cup serving of roughly 150 ml:
Six Gatorade cups at 150 ml = approximately 900 ml of Gatorade
Ten plain water cups at 150 ml = approximately 1.5 litres of water
Total race fluid intake: approximately 2.4 litres
Sodium from Gatorade (at 450 mg/L working estimate): approximately 405 mg
Sodium from five gels (at 200 mg each): approximately 1,000 mg
Total in-race sodium intake: approximately 1,405 mg
That number mattered more after I got back to the hotel.
By chance, our hotel room in Prague had a bathroom scale. It was found by accident, in a room we were not supposed to be in, after a noise complaint and a midnight negotiation involving two pillows the size of small children. The bathroom scale that made this analysis possible was not planned. Nothing about that room was planned. I weighed myself before the race. Five hours later, I crossed the finish line, walked the half kilometre to the post-finish refreshment area, ate a banana, drank a cup of water, walked back to the hotel, and weighed myself again.
The scale read 2.7 kg lower than my pre-race weight — after drinking approximately 500 ml on the walk back to the hotel. That scale reading reflects the finish-line deficit minus the 500 ml already consumed. Adding that 500 ml back gives an estimated finish-line deficit of approximately 3.2 kg at the moment of crossing the line — before any post-race fluid. The table models the 2.7 L scale reading. The 3.2 kg figure represents the true finish-line state.
My Garmin 255 estimated approximately 5.1 litres of sweat loss over five hours. Garmin’s sweat loss estimate is not a laboratory measurement. It is an algorithmic figure based on user profile and exercise data. Peer-reviewed research published in Sports Health (2025) found Garmin’s sweat loss algorithm carries a mean absolute percentage error of approximately 33 percent overall — and approximately 39 percent in male runners specifically — with individual estimates ranging from several hundred millilitres under to several hundred millilitres over actual measured loss.1 That error rate applies to standard wearable users running with default profile inputs. Individual accuracy may be considerably higher for runners who regularly sync a Garmin smart scale, as the algorithm may incorporate longitudinal body composition data into its sweat loss estimates. I had been doing exactly that — sporadically, without knowing why it mattered — for approximately a year before Prague with a Garmin smart scale. The study’s core conclusion stands regardless: do not rely on the wearable estimate alone. Use a scale. Which is, as it happens, exactly what this piece is built on.
The simple fluid balance looks like this:
Out — Estimated sweat loss: approximately 5.1 litres (Garmin, with the caveat above)
In — Fluid consumed on course: approximately 2.4 litres
Out — Mid-race urination: approximately 200 to 300 ml
In — Post-race water and banana consumed before stepping on the scale: approximately 500 ml
Net deficit: 5.1 − 2.4 + 0.3 − 0.5 = 2.5 litres
The bathroom scale showed 2.7 kg loss. The 0.2 kg gap between the expected deficit and the scale reading is consistent with substrate oxidation and respiratory losses over five hours of running — the body burns fuel and exhales carbon dioxide, neither of which appears in a cup volume estimate. The numbers are honest. The scale and the watch tell the same basic story.
For a runner of my mass, 3.2 kg represents roughly 3.8 percent body mass loss. That substantially exceeds the American College of Sports Medicine’s commonly cited guideline of limiting loss during exercise to approximately two percent.2 It is worth noting that this two percent threshold remains actively debated in exercise physiology: meta-analytic work has suggested that mild dehydration below approximately two to three percent may not uniformly impair performance across all field conditions, and some researchers advocate drink-to-thirst strategies as an alternative to volume-based targets.3 I will return to the drink-to-thirst question when the sodium arithmetic makes the stakes clearer. Regardless of where the precise threshold sits, a finish-line loss approaching four percent exceeds any reasonable planning benchmark, in any framework.
The fact that I finished is not evidence that the system worked.
It is evidence that my body absorbed a cost the system was supposed to help me avoid.
All my fault, of course. I had not read the course map carefully enough. I had not thought about sodium seriously before the race. I had loaded carbohydrates for days and left electrolytes to chance. I had seen that estimated sweat loss number in Garmin’s Connect app and never put two and two together. And in the end, I had not paid attention to getting enough fluids back into my body on the course.
All of that was my mistake. One hundred percent.
The question this piece asks is a different one: if the race organiser knew how much sodium their drink contained, how much their volunteers poured into each cup, and what the difference between those two numbers meant for a runner still out there at hour five — who was responsible for making sure that runner knew it too?
After the race, something felt off.
Was eight electrolyte stations enough? What did the sodium math actually mean for a five-hour marathoner? Was I simply undertrained, or had the course delivered less than I needed to plan around?
The deep dive.
The rabbit hole.
Before artificial intelligence, what you are about to read would have been near impossible for a recreational runner to produce alone.
I am not a physiologist. I am not a sports scientist. I am someone who finished a marathon with heavy legs and questions he could not answer. Over two weeks, five AI systems — Claude, Grok, ChatGPT, Gemini, and Kimi — helped me navigate a literature that was always there, sitting in journals that no recreational runner in Corral K had a practical path through. Not by lecturing. By answering each question in a way that showed me how to find the next paper, read the next study, ask the next question. The science was always there — in the New England Journal of Medicine, in ACSM position stands, in peer-reviewed papers on sweat sodium variability. It was never missing. It was just on the other side of a wall that most runners never had reason to climb.
Before this, getting from “my legs felt heavy at km 35” to a station-by-station plasma sodium model, cross-validated against a bathroom scale and a Garmin algorithm, would have taken months of finding researchers, reading papers, and hoping an expert wrote back. It happened in two weeks because I could ask a question, get an answer, and follow it all the way down.
That is what you are reading. Not just a critique of a race. A demonstration of what is now possible when anyone — a runner, a patient, a parent, a person with a question they cannot answer — has enough curiosity to keep asking. The answers were always there. Buried in journals, locked behind terminology, waiting in libraries that went quiet when the question walked in the door. They required wizards to find. They do not anymore.
I went back through RunCzech’s pre-race literature looking for guidance on sodium. Why it matters. How much a runner might need. What the alternating station design means for a runner expecting to be out there for five hours.
I found almost nothing. The word “minerals” appeared once, in a pre-race tip advising runners to alternate water with an isotonic drink — with no sodium target, no milligram, no concentration figure, no explanation of what “minerals” meant for a runner sweating through five hours of heat. That was it. That was the entirety of the guidance. They saw the gap. They named it in one word. And then moved on to the banana quantities.
There is a distinction worth stating plainly. Fault requires prior knowledge — you cannot be at fault for not knowing something you were never taught and never told. I am at fault for not reading the course map carefully enough. That error is in this piece and it stays there. But I am not at fault for not understanding sodium physiology in endurance running. I am forty-two years into this sport and I never encountered this information through a race, a club, a coach, or a registration package. That is not carelessness. That is the state of what the sport communicates to recreational runners. Responsibility, by contrast, belongs to the party with the knowledge. RunCzech knows exactly what their course delivers: the station spacing, the drink concentration, the cup size, the alternating design, and what a five-hour runner in warm conditions will face by the time they reach km 33. A runner in Corral K knows none of that. The asymmetry is total. When one party holds all the relevant information and the other holds none, the moral weight of the knowledge gap falls on the party that could have closed it but did not. The knowledge gap and the design gap are the same gap.
The race materials told me where the stations were. They told me what products would be available. They did not tell me why sodium matters during an endurance event, or what the physiological consequences of under-replacing it might be for a runner of my size, pace, and expected time on course.
Caveat emptor. I understand. Every runner signs a waiver. Every runner accepts personal responsibility for their preparation.
But no one at registration checks whether each of the 11,000 participants understands sodium and hydration dynamics as they apply to their own body. They take your entry fee and hand you a bib. The responsibility transfer is total and the information transfer is minimal.
It would cost almost nothing to say: based on your declared finish time, your expected sweat loss is approximately X litres. You will likely need approximately Y milligrams of sodium during the event. Here is what the course provides. Here is what you may need to carry. Adjust for race-day conditions.
That is not pampering. That is the information a runner needs to make responsible decisions about their own body before they cross the start line.
The Reply That Changed the Question
On May 4, 2026 — the morning after the race — I sent a formal written safety complaint to RunCzech, copied to World Athletics. I identified myself by bib number, corral, finish time, and placement. I framed the complaint explicitly as a runner safety concern, not a personal grievance about my result. I raised six specific issues: the difficulty of identifying Gatorade at pace due to inadequate signage and indistinguishable cups; the apparent dismantling of the km 33.5 station while a substantial number of runners were still on course; the absence of visible finish-line recovery nutrition; the absence of cooling sponges in warm race conditions; the three runners I personally observed collapsed or incapacitated on course, one requiring a confirmed ambulance response near km 40; and a medical communication gap I encountered at approximately km 28, where a course runner I had assumed was a medical professional — identified by a green flag and white cross — indicated he spoke only Spanish and could not communicate with me about a runner I had observed in distress. I requested formal acknowledgment, deployment and closure records for the km 33.5 station, total medical incident data, official starter and DNF statistics, and a commitment to review hydration, cooling, signage, and finish-line recovery protocols ahead of future events.
RunCzech replied in detail. Their response did not convince me that my concerns were imaginary. It clarified the structure of the problem.
A note on the Running Doctors programme. Based on publicly available finish data, the confirmed Running Doctor finishers completed the course between 4:03 and 5:05. With approximately 1,385 runners finishing after the 5:05 mark — still out on the course in peak afternoon heat, the furthest from the finish line, the most physiologically exposed — the coverage available to the slowest portion of the field cannot be confirmed from public records alone.
The deployment details of the two non-finishers and one participant whose bib number was not legible in available photographs remain unknown. One of the three may have been running with the back-of-pack field. One may have stopped to assist a runner and withdrawn from the race to do so — which, if true, would be exactly what the programme was designed for. We do not know. The deployment records required to answer that question were among the items formally requested in the complaint submitted to RunCzech on May 4, 2026. No response to that specific request has been received.
What is known: every confirmed Running Doctor who crossed the finish line did so ahead of the 1,385 runners still on the course. The green-flag, white-cross runner encountered at approximately km 28 — who indicated he spoke only Spanish and could not assist with a runner observed in distress — carried neither the red flag nor the “Running Doctors” branding visible in official RunCzech race photographs. Whatever role that runner was performing, it was not the Running Doctors programme.
RunCzech also provided a photograph in a private communication, offered as evidence that stations were clearly marked. The image showed a heavily staffed mid-race station, likely around km 21, with approximately 28 visible volunteers, Mattoni signs on the table fronts, and Gatorade signs farther along the line.
To RunCzech, this appeared to prove that the stations were clearly marked. To me, it demonstrated the opposite.
The signs were low, on the front of the tables. The runner’s visual field was cluttered with volunteers, cups, bodies, boxes, shadows, sponsor logos, and motion. There was no obvious overhead wayfinding that would allow a tired runner approaching at pace to clearly distinguish water from Gatorade before entering the congestion of the station.
A logo visible in a photograph is not the same thing as functional clarity for a runner. Aid station signage should be designed for the runner’s eye, not the photographer’s lens.
The cups themselves tell the full story. RunCzech’s water cups were black and white — Mattoni branding. The Gatorade cups were white and black — unknown branding. Both cups were the same palette. The same contrast. The same visual noise, in different arrangements, held in different hands, on the same tables, in the same chaos.
A runner approaching at pace, after four hours of fatigue and heat, cannot distinguish Mattoni-branded black-and-white water cups from unknown-branded black-and-white Gatorade cups. They are the same colours. That is not a signage problem. That is a design failure.
White for water. Green for Gatorade. One colour change. One decision. That is not a design brief. That is a description of what should have already been there.
The photograph also did not reflect what I saw at 33.5 km — one volunteer under a bridge pouring water from a bottle, one table standing, at least two being dismantled while runners were still arriving. A well-staffed mid-race station does not answer the concern about late course station function for slower runners. The front and middle of the race can look organized. The safety test happens later.
RunCzech stated that the 33.5 km station was water only. They stated that the 37.9 km station was water only. They stated that the final full refreshment station was at 39.7 km. They stated that no station ran out of water, but acknowledged there was likely a temporary shortage of bottled water at 33.5 km, with reserve water available from a tanker. They stated that sponges were not provided, citing post-Covid hygiene concerns. They stated that runners had to walk several hundred metres after the finish to reach the final refreshment area.
RunCzech provided aggregate medical treatment figures in a private communication. Those figures, without a denominator of total starters, DNS (Did Not Start) runners, or DNF (Did Not Finish) runners, cannot describe the full field experience — which is exactly the point.
What RunCzech did not provide were total registrants, starters, DNS figures, DNF figures, or where DNFs occurred. They also did not provide the electrolyte cup size, expected pour volume, whether the Gatorade was bottled ready-to-drink or mixed into water, or how much volunteers were instructed to pour per cup.
The denominator question got sharper a few days after the race. On May 8, 2026, RunCzech sent participants a post-race email — a private communication to registered runners — that opened with: “This was the Vodafone Prague Marathon 2026! 31st edition. 11,800 runners. Over 100 nationalities. And throughout the entire weekend, including the non-competitive runs such as the Lavazza Active Breakfast Run, dm family mile, and dm bambini run, more than 16,000 participants pinned on a race bib.”
The construction is deliberate. The 11,800 is the marathon. The 16,000 is the full weekend, including the non-competitive Saturday events that RunCzech explicitly enumerates. The word “And,” followed by “throughout the entire weekend,” distinguishes the two figures.
11,800 minus 9,066 finishers equals 2,734 runners — approximately 23 percent of the participation figure.
That is not a DNF rate. It is an unexplained gap. It is worth stating the most innocent explanation plainly: a meaningful share of those 2,734 runners may simply never have arrived in Prague. High DNS rates are common in international marathons, where travel disruptions, pre-race injuries, and last-minute deferrals routinely account for five to ten percent of registered fields. If DNS runners explain the majority of the gap, the picture changes considerably. Whether it reflects runners who did not start, runners who started and did not finish, chip failures, disqualifications, or some combination is exactly what the unpublished data would resolve. Many major endurance events provide fuller post-race accounting, including starter counts and non-finisher breakdowns. At minimum, starter and finisher counts are basic operational denominators. The gap between participants and finishers is not an unusual number to disclose.
The timing data makes the back of the field impossible to dismiss. The first four-hour finisher placed 3,747th — meaning more than 5,300 official finishers came after the four-hour mark. The first five-hour finisher placed 7,476th — with approximately 1,600 runners still behind them. The first six-hour finisher placed 8,792nd — with approximately 270 runners still on course. (Ordinal placements verified from the RunCzech official results database, Vodafone Prague Marathon 2026.)
Those runners were carrying the greatest cumulative heat load, fluid deficit, sodium deficit, and time on feet. They were precisely the runners most dependent on late-course hydration, clear signage, practical electrolyte access, and post-finish recovery.
The right question is not: “How many runners fell because of this?”
The right question is: “Why can we not tell?”
RunCzech’s reply changed the question. It was no longer: why did I not find Gatorade where I expected it? It became: what does this aid station model actually deliver to a five-hour runner, and what does a runner need to know to plan around it?
That is when I did the math.
The Half Cup Problem
To understand why the alternating-station design creates a safety problem for back-of-pack runners, three lines of arithmetic need to run in parallel: estimated sweat loss, the fluid volume required to stay within a reasonable dehydration margin, and the sodium required to prevent dilution while meeting that fluid target. When the drink provided on course is too dilute to satisfy both the fluid and sodium targets at realistic consumption volumes, the runner faces a structural choice between two risks. That is the half cup problem — and the table near the end of this section makes it visible in three rows.
Sodium is the main electrolyte in the fluid outside the body’s cells. It helps hold water in the bloodstream and extracellular space, supports nerve signalling and muscle contraction, and governs the body’s ability to keep fluid in the right compartments while under stress. When you sweat, you lose water and sodium together. If a runner replaces fluid volume with plain water but not sodium, blood sodium is diluted, potentially contributing to hyponatremia — a condition that in serious cases impairs brain and nervous system function.4 5 This risk has been studied at the population level: a landmark study of Boston Marathon finishers found that 13 percent of a sampled field met the clinical threshold for hyponatremia. The study found that weight gain during the race, longer race time, and BMI extremes were associated with hyponatremia on multivariate analysis, while the composition of fluids ingested — water versus sports drink — was not independently associated with hyponatremia. The study also noted that commercial sports drinks were too dilute in sodium to offset the risk from large fluid volumes.6
The implication for course design is important: it is not enough to provide sports drink. The sports drink must be concentrated enough to deliver meaningful sodium at realistic consumption volumes.
If a runner loses large amounts of sweat and under-replaces fluid, the risk runs the other direction: dehydration, rising heart rate, heat strain, and collapse. All runners face these constraints simultaneously — the question is not which risk exists, but how the course design creates conditions for managing both.
Sweat sodium concentration varies dramatically between runners. Two runners can run the same race, in the same heat, at the same pace, and lose very different amounts of sodium per litre of sweat.7 That is why electrolyte access is not cosmetic. It is part of the safety margin, especially for slower runners on course for five or six hours.
The arithmetic
My Garmin watch and Garmin’s Connect app estimated approximately 5.1 litres of sweat loss over five hours. Cross-checked against the bathroom scale, this is a reasonable order of magnitude. A practical low, medium, and high range for sweat sodium concentration is approximately 400, 700, and 1,000 mg per litre of sweat. [See note 7]
At 5.1 litres:
Low sodium sweater: approximately 2,040 mg sodium lost
Medium sodium sweater: approximately 3,570 mg sodium lost
High sodium sweater: approximately 5,100 mg sodium lost
The goal during a marathon is partial replacement — enough sodium to support fluid retention, reduce the risk of excessive dilution, and preserve a physiological safety margin until full recovery. For a medium sodium sweater over five warm hours, a practical in-race planning target is roughly 1,700 to 2,450 mg, with approximately 2,000 mg as a simple working figure. This is not a formal clinical guideline; it is a planning estimate derived from my estimated sweat losses and the ACSM sodium range for exercise fluids lasting more than one hour. [see note 2] Individual needs vary, and runners should test any such target in training.
At an estimated sweat sodium loss of 3,570 mg, a target of 2,000 mg represents approximately 56% in-race replacement. ACSM does not recommend complete replacement during exercise — the goal is to support blood sodium and fluid retention, not match losses milligram for milligram. The remaining deficit is restored in the hours following the race through normal food and fluid intake. In a hot race with significant fluid losses, however, 2,000 mg of sodium is doing its job in a smaller volume of blood than the planning model assumes. The margin shrinks. That is an argument for aiming toward the higher end of the planning range — not against the target, but for taking it seriously.
Commercial sports nutrition planning services validate this order of magnitude — though their financial interest in the conclusion is worth naming. Precision Hydration, a UK-based firm offering personalized electrolyte planning and selling the products that fill the gap they identify, recommends approximately 1,000 mg/L sodium and roughly 750 ml/hr fluid intake for a runner matching this profile — a sodium concentration more than double the working estimate used for Prague’s Gatorade Isotonic, and a fluid rate consistent with the 3.4 litre planning figure used throughout this piece. They are likely right. They are also selling capsules. The information and the product are not separable, and that context belongs on the table. It does not invalidate the numbers — they are consistent with ACSM guidance and the arithmetic in this piece. It does mean the numbers come with a commercial interest attached, and readers should weigh them accordingly.
Here is the logic behind it. If my estimated sweat loss was about 5 litres, and the goal is to avoid finishing more than about 2 percent below starting body mass, then my practical race fluid target was roughly 3.4 to 3.5 litres. If that fluid contains 500 to 700 mg sodium per litre — the ACSM recommended range for exercise lasting more than one hour [see note 2] — the sodium delivered would be roughly 1,700 to 2,450 mg, which brackets the 2,000 mg planning estimate.
The physiological catch-22
This is where the course design creates a structural trap.
My own data shows the dehydration half of it. I finished approximately three percent below starting body mass, with an estimated fluid deficit of nearly 2.5 litres. My experience was under-replacement, not over-replacement. But the only way for a runner without supplemental sodium to obtain approximately 2,000 mg of sodium from the on-course Gatorade Isotonic — at a working estimate of 450 mg/L — would have required consuming approximately 4.44 litres of that drink. That does not exceed total estimated sweat loss, but it substantially exceeds the conservative fluid-replacement target of 3.4 litres used in this analysis. A runner trying to solve the sodium problem through volume alone would be consuming far more than a conservative replacement target allows — at a small number of stations, in bolus volumes that are operationally unrealistic at marathon pace. In a runner who has been losing sodium for five hours, that excess volume arrives diluted, narrowing the margin against the dilutional hyponatremia described earlier. [see notes 4-6]
The course design does not simply reduce sodium opportunities. It forces the runner to solve sodium through volume. At a low sodium concentration, reaching a meaningful sodium target requires drinking a large amount of fluid at a small number of stations. That may still fall below total sweat loss, but it substantially exceeds a conservative replacement target and is operationally unrealistic at race pace. The result is not automatic danger. It is a narrowed margin — and for a five-hour runner in warm conditions, narrowed margins compound. The correct answer — a higher-concentration drink available at more stations — was not on the course.
The drink-to-thirst question
The 2015 Third International Exercise-Associated Hyponatremia Consensus [see note 4] emphasizes that drinking to thirst minimizes both dehydration and hyponatremia risk for most runners. That guidance is well-founded for a wide range of race conditions. But my own scale data provides one concrete illustration of why thirst may be insufficient for back-of-pack runners in warm, multi-hour conditions. I drank at every station, responded to perceived thirst throughout, and still finished approximately three percent below starting body mass — short of even a conservative fluid replacement target. Thirst perception in heat is imprecise, particularly after hours of exertion when cognitive resources are depleted. The drink-to-thirst strategy may provide adequate protection in cooler conditions or at faster race paces; under the heat load Prague runners experienced in 2026, the scale data suggests it was not sufficient, at least for runners in my corral. This does not invalidate drink-to-thirst as a principle. It does suggest that course design cannot rely on it as a substitute for providing adequate sodium-containing fluids.
My backup plan and what it cost
When I picked up my race kit at the RunCzech expo, I bought Enervit Carbo Gel C2:1 Pro — formulated with extra sodium for hot weather endurance use, 200 mg of sodium per gel. I took five gels. That gave me approximately 1,000 mg of sodium independent of the race. I had a sodium backup plan in my pocket. Many runners may not have.
For the arithmetic, I use a conservative working estimate of 450 mg sodium per litre for the Gatorade Isotonic served at the race. A note on this estimate: the European Gatorade Isotonic product typically contains approximately 420 mg of sodium per litre, which is slightly lower than 450 mg/L. If anything, this means my arithmetic is marginally generous to RunCzech — the true numbers for runners may be modestly more severe. If RunCzech used a higher on-course concentration, they can publish the mixing protocol and product source to correct this estimate.
Product category is not the same thing as delivered dose. RunCzech has not, to my knowledge, provided the exact on-course delivery details: bottled ready-to-drink versus powder or concentrate mixed into water, dilution protocol, quality control, cup volume, expected pour volume, or late-race replenishment procedure. If those details produce different numbers, they are welcome to publish them.
Cup capacity is not runner intake
The water cups visible in RunCzech Instagram photography appear to be marked 0.3 L. A 300 ml cup is not 300 ml delivered to a runner. If filled halfway, it is about 150 ml. If grabbed at speed, tilted, squeezed, spilled, sipped, or dumped over the head, the amount actually swallowed may be less. That is the half cup problem.
At 150 ml per practical half cup, even with my five sodium-containing gels, I would still have needed roughly one to two and a half cups of Gatorade at every Gatorade station to reach the practical sodium range. That is with my gels.
For a runner without sodium gels, the math becomes much harder. To obtain approximately 1,700 to 2,450 mg of sodium from Gatorade alone would require approximately 3.8 to 5.4 litres — or three to four and a half cups at every full refreshment station. That is not a hydration plan. That is stopping for a picnic.
What the deterioration looks like, station by station
The following two tables trace what the arithmetic looks like in real time — one station at a time, across 5 hours and 6 minutes of running in the heat.
Both tables are modelled simulations for an 85 kg male runner completing the course in 5:06, using a medium sweat rate of 1 litre per hour and sweat sodium concentration of 700 mg/L — the same assumptions used throughout this piece. They are planning models, not clinical measurements. Individual sweat rates, sodium losses, and fluid needs vary widely.
The final column — Concentration pressure (directional) — uses a simple symbol system to show the net directional pressure on sodium-fluid balance at each station. It does not estimate actual blood sodium, which depends on renal handling, hormonal response, urine output, and absorption that no spreadsheet can capture. The symbols show trajectory, not chemistry.

Table 1 is what I actually did: one cup per station, gels placed across both station types without knowing the alternating design.
Table 2 is what a runner armed with complete advance knowledge of the course could have done: two cups at every station, every gel placed at a water-only station to leave every Gatorade station free for maximum sodium intake.
Methods note: The following tables are planning models, not physiological measurements. They assume an 85 kg runner, 5:06 finish time, 1 L/hr sweat rate, and 700 mg/L sweat sodium. Stations are distributed over the first 4:48 of the race, with the last aid station at approximately km 39.7 and the finish at km 42.195. The finish row adds continued sweat loss over the final ~2.5 km with no further fluid intake. Urine loss (~200–300 ml) is not embedded in the table — it is handled separately in the prose and accounts for the remaining gap between the table’s finish deficit and the bathroom scale result. Gatorade Isotonic sodium is estimated at 450 mg/L as a working figure, not a confirmed delivered dose. Practical cup intake is estimated at 150 ml per cup for Prague tables and 220 ml for Table 4. The concentration pressure column shows directional pressure only — it does not estimate actual blood sodium.
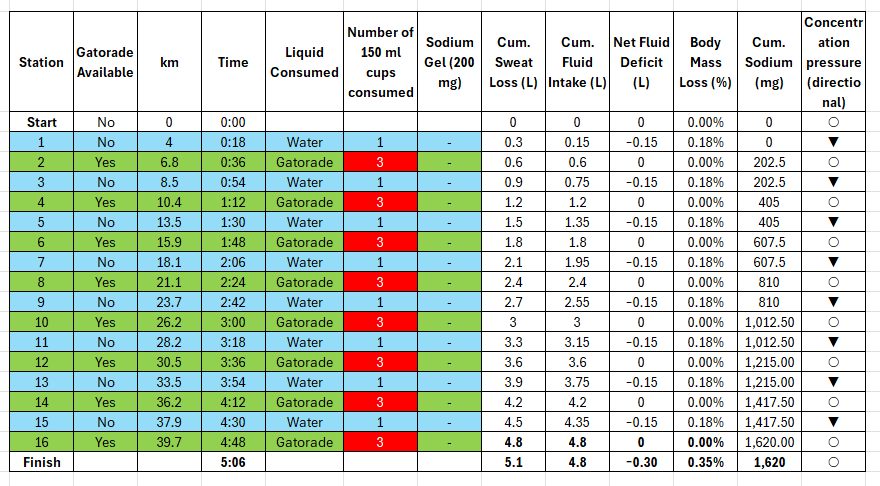
Table 1: Actual Prague Race (1 cup per station)
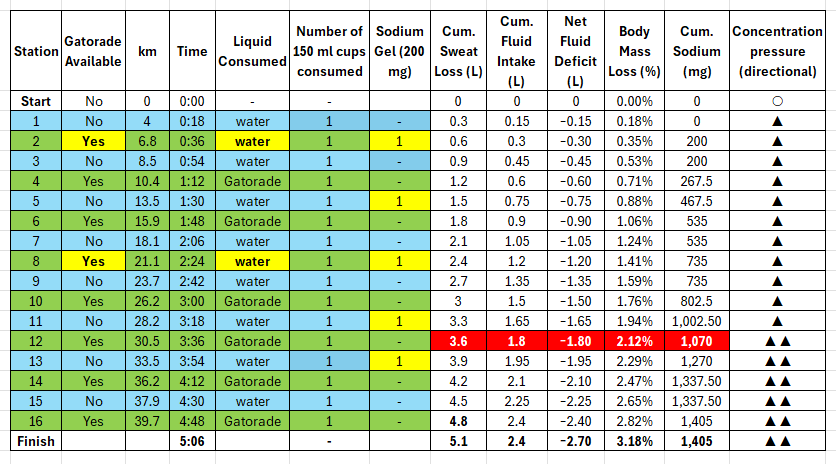
Colour key: Blue cells in the Liquid Consumed column indicate water was taken at that station. Green cells indicate Gatorade was consumed. Yellow cells in the Sodium Gel column mark stations where a carbohydrate gel (200mg sodium) was taken. The red row at Station 12 marks the crossing of the 2% body mass loss planning threshold.
The “1” in every row of the cups consumed column is the half cup problem in numbers. One cup per station. Sixteen times. From the first kilometre to the last.
Green highlights in the Gatorade Available column at Stations 2 and 8 show that Gatorade was present — but the Liquid Consumed column shows water was chosen at both. The yellow gel column confirms gels were taken at those same stations. Both were missed double-sodium opportunities: the gel’s 200mg was taken; the Gatorade’s additional 67.5mg was not. Combined: 135mg of sodium left on the course at stations where it was available.
Green highlights at Stations 5, 11, and 13 with blue liquid consumed mark water-only encounters where a gel provided the only sodium. Right call, wrong reason — the sodium was fortunate product selection, not deliberate planning.
The red row at Station 12 (km 30.5, 3:36) is where the system stopped keeping up. Concentration pressure shifts from ▲ to ▲▲. The five rows below it, through the finish, never recover.
The table is a model. The following chart was the race.
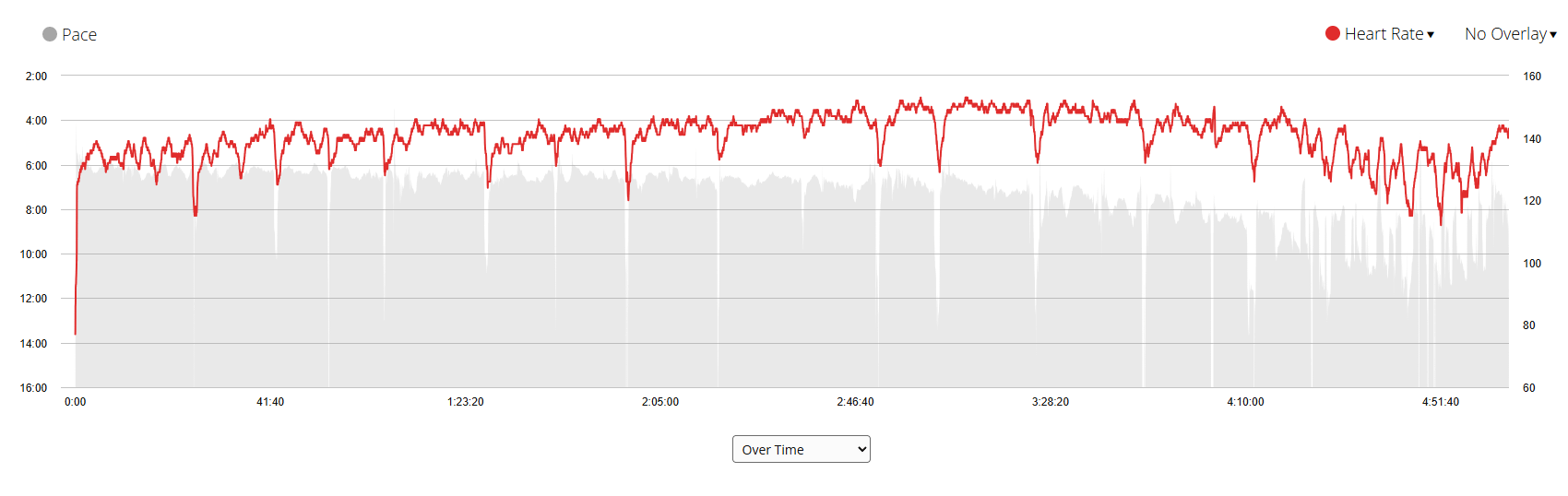
Garmin Connect combined chart, Vodafone Prague Marathon 2026. Grey area: pace (min/km), plotted so that higher on the chart means slower. Red line: heart rate (bpm), right axis. Both plotted over time from start to finish.
The two data series tell the same story in opposite directions. Through the first half of the race, pace holds — imperfect but controlled — while heart rate climbs gradually. From approximately 3:28 onward, pace becomes increasingly erratic and progressively slower, never returning to the level of the opening kilometres. Heart rate continues to drift upward through the same period, peaking in the final third of the race and remaining elevated through the finish. The corrected model places the 2% body mass loss planning threshold at Station 12, approximately 3:36 into the race. The Garmin data is consistent with that story: the cardiovascular system was compensating for a fluid deficit that had been building since the first kilometre, and by the time the legs noticed, the threshold had already been approached. Pace fell. Heart rate climbed. Neither recovered. They do not prove causation, but together they fit the fluid-deficit explanation better than I understood at the time.
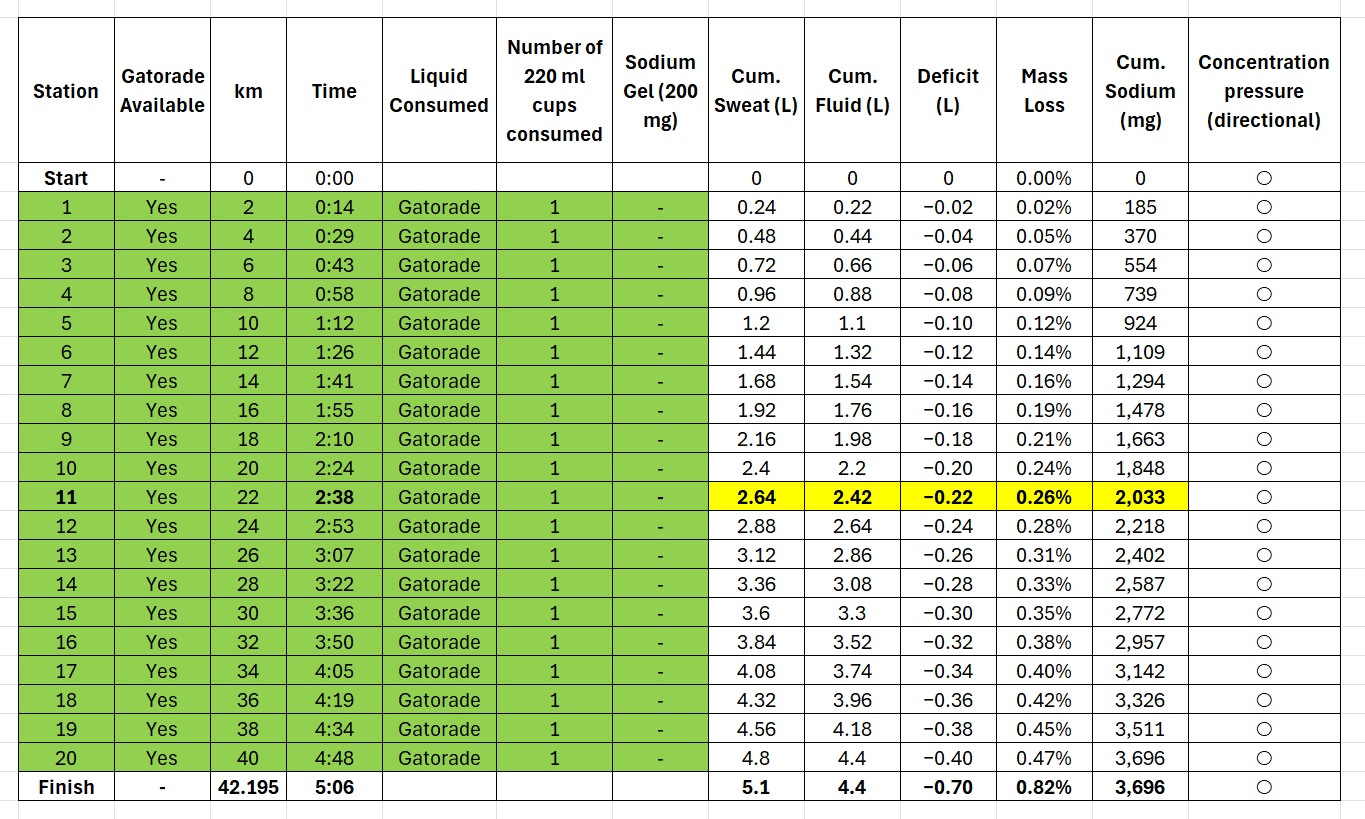
Table 2: Optimized Strategy — Gels on Water-Only Stations, 2 Cups per Station
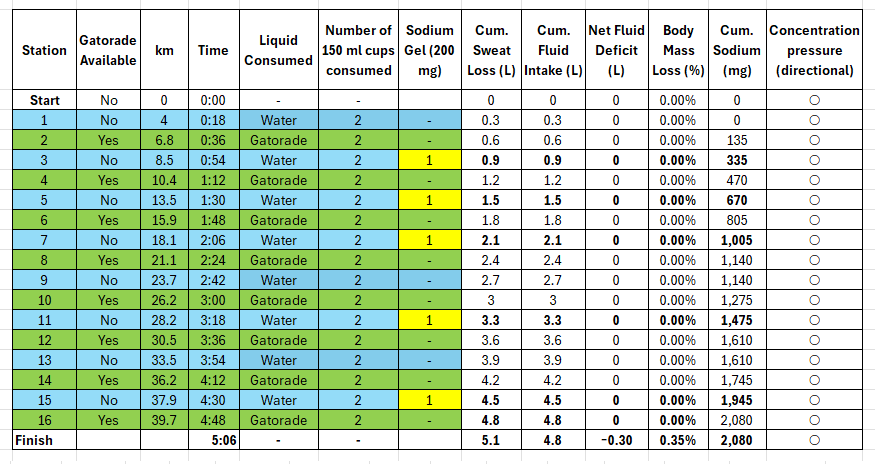
Colour key: Blue = water consumed. Green = Gatorade consumed. Yellow in the Sodium Gel column = gel taken at that station.
The “2” in every row of the cups consumed column is the only change from Table 1. Same course. Same stations. Same drink. One more cup. Two cups of whatever was available — water or Gatorade — at every stop.
Gels are now placed at water-only stations (3, 5, 7, 11, 15). Every Gatorade station gets Gatorade. Every water station gets a gel. No overlap. No missed opportunities. 135mg recovered.
The Net Fluid Deficit column holds at zero from start through Station 16. Body mass loss: 0.00% through the entire race. The finish row shows −0.30L and 0.35% — the unavoidable consequence of the final 2.5km with no aid station until the recovery area - 460 m from the finish line. The concentration pressure column shows ○ throughout. Every row. Including the finish.
I could have run this race better. With the Mattoni water. With the Gatorade Isotonic at 450mg/L. With my gels. The course that existed was enough — if I had known what to do with it. I didn’t know. I do now.
Table 3: The Sodium Gap — No Gels, Best Realistic Effort
"What an 85 kg, 5-hour, medium sodium sweater may have required to consume in order to stay reasonably hydrated on RunCzech's course on May 3, 2026. No gels."
A runner without sodium gels faces a much harder problem. The only sodium on the course comes from eight Gatorade stations. The following table models the most realistic disciplined effort: one cup of water (150 ml) at every water-only station, three cups of Gatorade (450 ml) at every Gatorade station. No gels.
Assumptions: 85 kg runner, 1 L/hr sweat rate, 700 mg/L sweat sodium, 5:06 finish time. 1 cup water (150 ml) at each of 8 water-only stations; 3 cups Gatorade (450 ml) at each of 8 Gatorade stations. Total fluid to station 16: 4.80 L. This is a model, not a clinical measurement. The finish row reflects continued sweat loss over the final ~2.5 km from the last station to the finish line, with no further fluid intake.
Colour key: Light blue = water consumed. Green = Gatorade consumed. Red cells in the cups consumed column = three cups taken at that station.
The red “3” at every Gatorade station is the story. Three cups of Gatorade Isotonic — 450ml — at every Gatorade station. Not a sip. Not one cup. Three. At race pace. Stomach working for four hours. The next station 2.6km away. That is what fluid balance requires when the drink concentration is 450mg/L instead of 840mg/L.
Water stations: 1 cup, ▼. Gatorade stations: 3 cups, ○. The alternating pattern is perfectly regular — the deficit returns to exactly 0.00% at every Gatorade station, then slips back to −0.15L at every water station. The runner is never in danger. But can never build a surplus. The finish row shows 0.35% body mass loss and ○ — the same outcome as Table 2’s optimised strategy. But look at what it cost to get there.
And yet: total sodium at the finish is 1,620mg — 380mg short of the 2,000mg planning target. Three cups of Gatorade at every Gatorade station, for five hours, executed without error. Still short. That gap is structural. It cannot be closed by trying harder. It can only be closed by a more concentrated drink.
That is the sodium gap. Not a disaster. Not hyponatremia. Just a quiet, accumulating shortfall that the course design made structurally unavoidable for a runner without supplemental sodium — regardless of how carefully they drank.
One thing this table states quietly without fanfare: achieving even this outcome required the runner to consume three cups of Gatorade — 450 ml — at each of the eight Gatorade stations. That is not a sip. That is nearly half a litre, grabbed at pace, in a crowd, while breathing hard, with a stomach that has been working for two, three, four hours. At aid stations that offered no overhead signage to identify which cups were which. In black-and-white cups that looked almost identical to the water cups beside them. The model assumes perfect execution. The race did not provide the conditions for it.
Table 4: What the Course Could Have Delivered
Now remove everything Prague got wrong — the alternating design, the low-concentration drink, the eight electrolyte-free stations, the planning burden — and replace it with what the arithmetic actually requires. Twenty stations. All Gatorade Endurance. No gels required. No strategy required.
Assumptions: 85 kg runner, 1 L/hr sweat rate, 700 mg/L sweat sodium, 5:06 finish. 20 stations equally spaced to km ~39.7 (4:48), with finish at 5:06. 220 ml Gatorade Endurance (840 mg/L, 184.8 mg sodium) at every station. Finish row reflects continued sweat loss over the final ~2.5 km with no further fluid intake. 220 ml is just under three-quarters of Prague’s standard 300 ml cup — less than Prague asked runners to drink, more than Prague’s design could ever deliver.
Every row is ○. The concentration pressure column never moves. The deficit grows by only 0.02 L per station — the runner is replacing 92% of sweat loss at every stop without stopping, without strategy, without calculation. The 2,000 mg sodium planning target is crossed at station 11, at 2:38 into the race — before the halfway point, with nine stations still to go. The runner arrives at the finish line at 0.82% body mass loss, well under the 1% target, with 3,696 mg of sodium replaced — 126 mg above total sweat sodium losses. Not short. Not dangerous. Not a planning problem the runner had to solve alone.
This is why the drink concentration matters more than the drink volume. Gatorade Endurance at 840 mg/L carries more sodium per litre than sweat at 700 mg/L — so every litre consumed replaces more sodium than was lost in the corresponding sweat. The runner does not need to think about sodium separately from fluid. The drink handles both simultaneously. Prague’s Gatorade Isotonic at 450 mg/L carries less sodium per litre than sweat. Every litre consumed replaces only 64% of the sodium lost in the same sweat. The runner can never catch up through volume alone. That is the entire argument in three numbers: 840, 700, 450.
The cup: 220 ml. Just under three-quarters of Prague’s 300 ml cup. Less per station than Prague’s cup was designed to hold. More than Prague’s system could ever deliver.
Table 5: Four scenarios, One Verdict
The Difficulty to Consume column names the human reality that arithmetic alone cannot capture. Tables 1 and 4 both require the same effort from the runner: one cup per station, no gel strategy, no planning document. The natural, effortless thing a runner does at an aid station — grab a cup and keep moving. Table 1 ends at 3.20% mass loss and ▲▲. Table 4 ends at 0.82% and ○. Same behaviour. Completely different outcomes. The runner did not fail. The drink failed the runner.
Table 3 requires Heroic effort — three cups of Gatorade at every Gatorade station, for five hours, at race pace, in heat, with a stomach that has been working since km 4. And it still ends 380mg short. The course asks for Heroic and delivers insufficient sodium regardless.
The table below shows what each course design actually delivers.
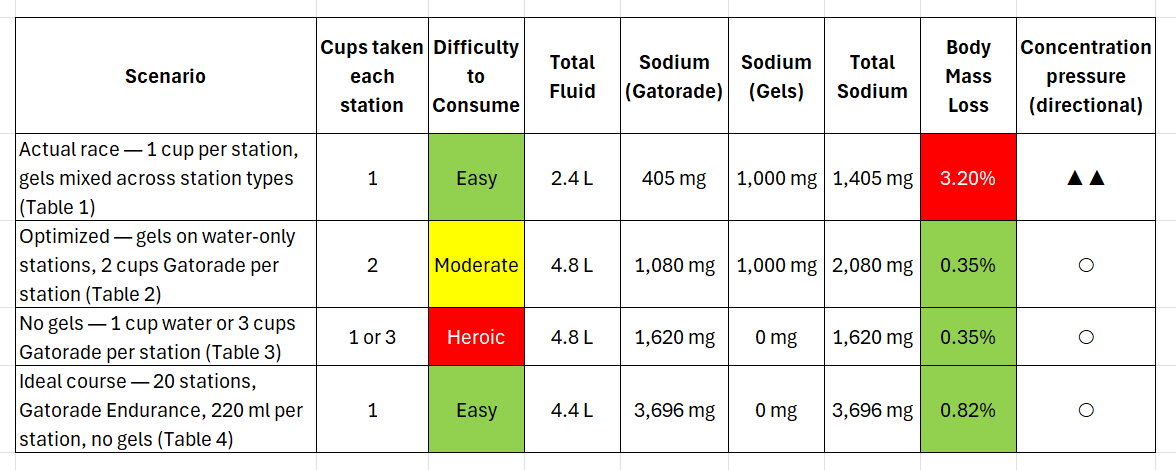
Note: Sodium estimates use 450 mg/L for Prague Gatorade Isotonic (Tables 1–3) and 840 mg/L for Gatorade Endurance (Table 4). Body mass loss values reflect the finish line after continued sweat loss over the final ~2.5 km from the last station. All figures are planning model estimates, not clinical measurements. Concentration pressure column uses directional symbols only — see symbol legend in table setup section above.
Table 5 tells four scenarios in two columns that matter most — Difficulty to Consume and Concentration pressure. The actual race: Easy effort, ▲▲ outcome. The optimized strategy: Moderate effort, ○ outcome — but only available to a runner who had decoded the pre-race materials and understood the math behind them. Not just which stations had Gatorade. But why plasma sodium rises as you lose weight to sweat. Why adding too much plain water dilutes it in the other direction. Why a 2% drop in body mass triggers a cascade the legs feel long before the mind recognises it. That knowledge was not in RunCzech's literature. It was not in any race briefing I have ever received in 42 years of running. It took two weeks and five AI systems to find it. The no-gel effort: Heroic effort, ○ outcome, with 380mg of sodium still missing at the finish. That gap is structural. It cannot be closed by trying harder. And the ideal course: Easy effort, ○ outcome, 3,696mg sodium, no planning required. The runner using Table 4's course does less work, faces fewer decisions, and finishes better — because the infrastructure was designed around what the runner actually needs.
A note to the reader: these tables are not prescriptions — they are a worked example. The inputs that drove every number in this piece are four: your expected finish time, your body weight, your sweat rate, and your sweat sodium concentration. Change any of them and the table changes with it. A runner of any size, any pace, any sweat profile can build their own version of Tables 1 through 4 using nothing more than a bathroom scale before and after a long training run and the same arithmetic used here. That is where the knowledge starts. Not in a lab. On your own bathroom floor.
A runner cannot build a reliable hydration plan from symbols, branding, and assumptions. A real hydration plan requires numbers: cup size, typical poured volume, delivered sodium concentration, whether the drink was bottled or mixed, dilution protocol, and late-race supply commitments. The station map tells the runner where the cups are. It does not tell the runner what is in them, or how much is needed.
That is the gap.
The 22,000 Litre Question
RunCzech’s public pre-race material stated that more than 56,000 litres of water and more than 22,000 litres of isotonic drink would be available at the stations.
That sounds enormous.
Using the full marathon field figure of 11,800 registered runners — acknowledging that the 22,000 litres was likely shared across all race distances and event formats — 22,000 litres represents a theoretical maximum of approximately 1.86 litres per marathon runner if allocated exclusively to that group. Compressed into only eight Gatorade stations, that theoretical allocation equals approximately 230 ml per runner per Gatorade station — roughly one and a half half-cups at each stop.
But the “1.86 litres per runner” figure describes what the race made available. It does not describe what the runner needed. Even if every drop were consumed perfectly, that per-runner allocation falls short of the physiological need for a warm, five-hour race.
Two different arithmetic problems sit behind the same set of cups.
Table 3 confirms this arithmetic directly. The no-gel runner uses 3.6 litres of Gatorade — eight stations at three cups each — plus 1.2 litres of water at the eight water-only stations, for a total of 4.8 litres. The Gatorade component alone is nearly double the 1.86 litre per-runner allocation in RunCzech’s headline figure. And even at that level of disciplined effort, sodium reaches only 1,620 mg: 81 percent of a reasonable planning target. Adding plain water at water-only stations does not solve the sodium gap. It cannot. Plain water carries no sodium. That is before considering real-world station mechanics: three cups of Gatorade at each full refreshment station would require runners to slow down, grab multiple cups, drink them quickly, avoid collisions, and re-enter the flow. If large numbers of four, five, and six hour runners tried to do that, the refreshment stations would become bottlenecks.
The volume problem cannot be solved by determination alone. The runner cannot safely keep increasing fluid intake to chase sodium from a low-concentration drink. At some point, the strategy trades one risk for another: under-replacing sodium versus over-consuming fluid and narrowing the margin against hyponatremia. [see notes 4-6]
A five-hour runner cannot consume “event total litres.” He can only consume what is available in front of him, at the station he is passing, in the cup he can identify, while moving, fatigued, hot, and surrounded by other runners.
A warehouse full of Gatorade does not hydrate a runner at km 33.5.
A clearly marked cup in his or her hand does.
The Time Between Sodium Tables
A brief comparison matters here — not just between Prague and North American majors, but across the full range of major marathons, and across the full range of finish times.
The five races modelled below share one assumption: one cup per station, 150ml, no external gels. The runner does the natural, effortless thing — grabs a cup and keeps moving. The course provides whatever it provides. The question is what that actually delivers.
Table 6a: Fluid — Body mass loss at 1 cup per station (150ml), by finish time
Assumptions: 85kg runner, 1L/hr sweat rate. No gels, salt packets, or supplemental electrolytes — fluid replacement only. A finish at or below 2.0% body mass loss is the planning threshold used throughout this piece. ✓ = within threshold. ✗ = exceeds threshold. ⚠ = slight overhydration.
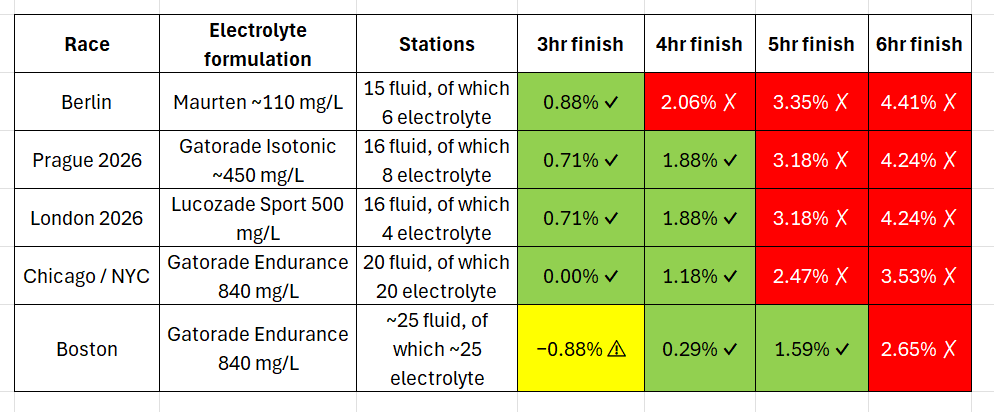
Not one race on this table is safe for a 6-hour runner at one cup per station. Berlin fails everyone running slower than 3 hours. Prague and London fail everyone running slower than 4 hours. Chicago and New York fail everyone running slower than 4:30. Boston — the only race with enough stations to protect a 5-hour runner — still fails the 6-hour runner. And a 3-hour runner at Boston drinks more than they sweat: mild overhydration, a different risk entirely.
Table 6b: Sodium — Percentage of sweat sodium losses replaced at 1 cup per station (150ml), by finish time
Assumptions: 85kg runner, 700mg/L sweat sodium. Sodium lost = finish time × 700mg/hr. Sodium delivered is fixed by course design regardless of finish time. The planning threshold used throughout this piece is approximately 56% replacement (2,000mg of 3,570mg lost for a 5:06 runner). ✓ = at or above threshold.
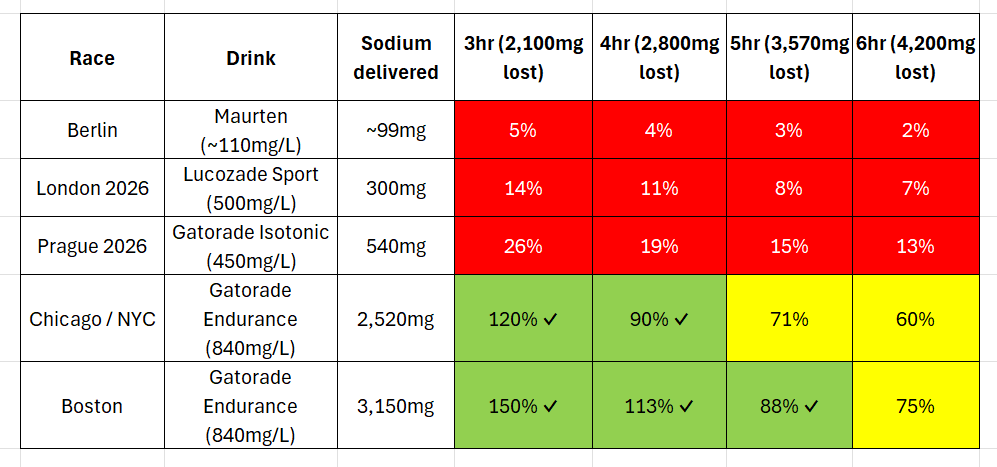
The sodium table reveals something the fluid table cannot. Course sodium delivery is fixed — determined by the number of electrolyte stations, the cup size, and the drink concentration. It does not change with finish time. But runner sodium loss scales directly with time on course: every additional hour adds another 700mg of sodium lost. The gap between what the course delivers and what the runner needs widens with every hour. A 6-hour runner at Berlin replaces 2% of their sweat sodium losses. Two percent. A 6-hour runner at Boston — the best-provisioned race on this table — replaces 75%, and still falls short. Not one race adequately replaces sodium for a 6-hour runner at one cup per station.
The back of the pack pays twice. More dehydration. More sodium deficit. Longer in the heat. The course infrastructure was set up for someone who finished hours ago.
Note: Berlin Maurten sodium (~110mg/L) estimated from available product specifications. London Lucozade Sport sodium (500mg/L) sourced from published product nutrition data. Prague Gatorade Isotonic (450mg/L) is a working estimate — the delivered concentration was not published by RunCzech. Boston and North American figures reflect published Gatorade Endurance specifications. Cup volume of 150ml is inferred from RunCzech Instagram photography showing a 0.3L cup filled approximately halfway; assumed consistent across races for comparison purposes.
The Vodafone Prague Marathon 2026 had 16 aid station encounters, with electrolyte drink at eight of them.
The Berlin Marathon complicates a simple Europe-versus-North-America contrast, but not in the way that might be expected. It provides Maurten Drink Mix at a small number of stations, but Maurten is formulated for carbohydrate delivery via hydrogel technology, not sodium replacement — its sodium concentration is minimal, and the company explicitly states there is no strong scientific evidence that athletes need to add electrolytes during activity. (Maurten FAQ, maurten.com/faq/general-product.) Sports nutritionist Meghann Featherstone, writing about World Marathon Majors course nutrition, is direct about what this means in practice: “The vomit at the 2023 finish line confirmed my suspicion that many runners did not get the memo to carry their own electrolytes — as nausea/vomiting is a common side effect of inadequate sodium intake.” Her recommendation for Berlin runners is equally plain: “You will likely need to carry all your fuel and electrolytes for the Berlin Marathon.”8 It is worth noting that nausea and vomiting in marathon finishers has multiple causes — GI ischemia, heat stress, and pacing among them — but Featherstone’s observation captures the operational reality: Berlin does not pretend to solve the sodium problem. It places that responsibility explicitly on the runner.
But there is a further problem that Berlin’s design does not acknowledge: Maurten’s product was not built for the runner most likely to need electrolytes.
Maurten’s hydrogel technology was built for the part of the field finishing in two to three hours — athletes where high-rate carbohydrate delivery under race intensity is the binding physiological constraint. For that athlete, in those conditions, Maurten’s FAQ position on electrolytes is scientifically defensible. The four, five, and six hour runner, sweating into peak afternoon heat and losing sodium for hours longer than that technology was designed for, is precisely the runner Maurten’s own FAQ identifies as someone for whom electrolyte discretion becomes relevant — and the runner their product was not built to serve.
Berlin is therefore not a counterexample to the problem described here. It is a more honest version of the same problem. London’s model is different again. The point is not that one continent has solved this and another has not. The point is that major marathons vary widely in electrolyte station density, drink concentration, and what the runner can realistically consume, and that some of the world’s most prestigious races leave back-of-pack runners to self-supply sodium entirely. That variance is visible, real, and worth a serious operational review by World Athletics and major marathon organizers.
The problem with fewer electrolyte stations is not only that runners receive fewer opportunities to drink sodium-containing fluid. It is that every electrolyte station has to do more work. More fluid per station. More sodium per station. More time between corrections. That matters most for slower runners.
What Was in the Cup
The number of sodium opportunities changes everything. And so does the concentration of sodium in those opportunities.
Some marathon sports drinks sit near the lower end of the ACSM’s recommended sodium range of 500 to 700 mg per litre. [2] For Prague, I use the conservative 450 mg/L working estimate. Gatorade Endurance Formula — the drink served at Boston, New York City, Chicago, and many other North American marathons — contains approximately 840 mg sodium per litre. (Gatorade product specification.) The actual sodium concentration of any tablet- or powder-based electrolyte drink depends on both the product formulation and the volume of water used to dissolve it — which is precisely why races should publish their mixing protocols. A tablet dissolved in 300 ml of water delivers a very different sodium concentration than the same tablet dissolved in 500 ml, and a runner cannot plan around a number that has not been disclosed.
That difference matters.
At 450 mg per litre, a runner trying to obtain 2,000 mg of sodium from the drink alone would need approximately 4.44 litres — about a litre more than the 3.4 litre fluid target. The two targets do not line up cleanly. The runner who drinks enough to hit the sodium target may exceed the fluid target. The runner who drinks only enough to hit the fluid target may under-replace sodium.
This is not specific to Prague. It is structural. The runner must carry sodium separately, accept under-replacement, or hope the course design gives enough frequent opportunities to adjust in small doses.
At 840 mg per litre, the math changes. To deliver 2,000 mg of sodium from a drink at 840 mg per litre requires approximately 2.35 litres — comfortably below the 3.4 litre fluid target. The runner can drink to thirst at Gatorade stations, add plain water at water-only stations to reach the fluid target safely, and hit both sodium and fluid goals without the two ever working against each other.
Put simply: Gatorade Endurance at approximately 840 to 870mg/L — depending on product format — is more sodium-dense than the sweat of a medium sodium sweater at the 700mg/L working assumption used throughout this piece. Every sip replaces more sodium than the corresponding sweat removed. Prague’s Gatorade Isotonic at 450mg/L is less sodium-dense than that same sweat. Every sip replaces less. That single difference — 840 to 870 versus 450 versus 700 in sweat — determines whether the drink is solving the problem or simply delaying it.
Gatorade Endurance is not magic. A heavy sweater with high sweat sodium concentration can still lose more sodium than the drink replaces. A runner can still overdrink. A runner still has to train and plan. But its operational safety value is clear: it distributes meaningful sodium through fluid across the course in repeated small doses, without requiring a tired five-hour marathoner to solve fluid volume, sodium replacement, station spacing, signage, and late-race cognition all at once.
At 1,000mg/L — the confirmed concentration of XACT Nutrition “Citrus Bang” for the 2026 Manitoba Marathon — the structural problem described in this section effectively disappears. To deliver 2,000mg of sodium requires only 2.0 litres of fluid: comfortably within the fluid target for any finish time. The two targets align naturally. A runner drinking to thirst at XACT stations is almost certainly replacing sodium at a rate that matches or exceeds sweat losses with every cup.
XACT at 1,000mg/L is the most sodium-dense drink in this analysis. More concentrated than Gatorade Endurance. More concentrated than any drink served at Boston, Chicago, or New York. At two cups per station — 180ml — Manitoba’s 15 stations deliver 2,700mg of sodium: enough to cover every finish time from 3 hours to 6 hours at the planning threshold used throughout this piece.
The cup is still half full. The station count has held for at least 28 years. But the drink — if mixed as confirmed — transforms Manitoba's sodium picture entirely. The race did not add stations. It changed what was in the cup. That one decision moved the Manitoba Marathon from the bottom of this analysis's sodium delivery table to the top.
That is the difference between a hydration system designed as infrastructure and one designed as a checklist item.
The Race I Thought I Knew
I have run in the Manitoba Marathon multiple times. I would love to call it Canada’s best marathon. But I only have a sample size of N=2, the other being Edmonton. Still, with all personal biases aside, I believe it is a premiere event.
What I did not know back when I ran my first race in 1993 — what none of us knew, because the science did not yet exist to tell us — was that the race was already failing some of its runners in ways no one could see from the finish line.
On Father’s Day 1995, the Manitoba Marathon started with more than 6,000 runners and ended with 193 finishers. The temperature reached 31°C. The humidity made it feel closer to 37°C. The race was stopped. Officials acted on what they could see: collapsed runners, dangerous conditions, a field that needed to come off the course. (The Hamiota Echo, July 4, 1995, p. 3.)
What they could not see was what was happening inside the runners still moving.
One finisher — 73rd overall in 3:43:56 — noted that near the 19-mile mark he had noticed swelling in his arms and hands. He had never before walked during a marathon. He slowed, walked periodically, and ran through water sprinklers set up along the way to cool himself.
At the 2025 Manitoba Marathon, at km 41.5 — less than a kilometre from the finish line — I came across a runner who had collapsed and could not feel his legs.
He did not finish. The finish line was right there.
Swelling in the hands during a marathon, or the sudden inability to feel one’s legs near the finish line — neither is proof of a specific condition. Both can have multiple causes. But in the context of extreme heat, prolonged exertion, and inadequate sodium guidance, both are at minimum consistent with the kind of physiological signals that marathon medicine would later learn to take seriously. A runner cooling himself with water sprinklers, arms and hands swelling at mile 19. A runner at km 41.5, legs gone, finish line in sight.
The body was sending signals. In 1995, nobody had the language to read them. By 2025, the language existed. The question is whether it travels.
The Almond Boston Marathon study — the paper that put hyponatremia on the marathon medicine map — would not be published for another ten years after 1995. The ACSM sodium position stand was twelve years away. The concept of exercise-associated hyponatremia as a clinical entity was not yet in the vocabulary of recreational running.
A course map published in the Winnipeg Free Press on June 20, 1998 — the year the Manitoba Marathon promised to be the biggest and best in its 20-year history, with approximately 8,000 contestants at the starting gate — shows approximately 16 hospitality stations along the full marathon route. (Winnipeg Free Press, June 20, 1998, p. 66.)
I ran that race. It was my first finish over four hours. I took one cup per station. I did not know why it was harder than it should have been. The tables in this piece now tell me what the course was delivering to a 4-hour runner that day, who wasn’t paying attention to sodium or getting enough water. For I certainly wasn’t at that time.
Manitoba Marathon: the 6oz cup
Assumptions: 85kg runner, 1L/hr sweat rate, 700mg/L sweat sodium, 90ml per cup (6 oz cup filled halfway, confirmed by race management), 1 cup per station. ✓ = within planning threshold. ✗ = exceeds threshold. 2025 station count confirmed from published participant handbook. 2026 station count and cup details confirmed by Manitoba Marathon race management, May 26, 2026.
At one cup per station, the fluid picture has not changed in at least 28 years. Manitoba delivered 1.44L at 16 stations in 1998. It delivers 1.44L at 16 stations in 2026. The fluid infrastructure is where it has always been. What changed is what was in the cup.
Table 7b — Sodium: % of sweat losses replaced at 1 cup per station (90ml):
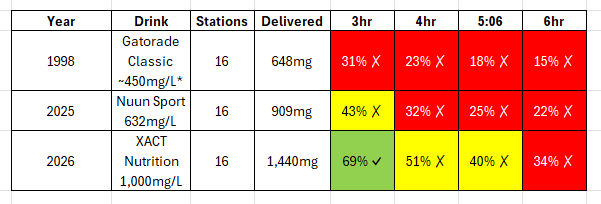
Gatorade Classic sodium concentration is an estimate. The drink served in 1998 is not confirmed from available documentation.
At 90ml per cup — a 6 oz cup filled halfway, as confirmed by race management on May 26, 2026 — one cup per station delivers 1.35L of fluid and 1,350mg of XACT sodium. That covers only 3-hour runners adequately on sodium, and leaves every runner short on fluid. Everyone finishing in 4 hours or more needs more than one cup per station.
The cup size revelation matters for a reason beyond arithmetic. The piece you are reading is called The Half Cup Problem. The cups at the Manitoba Marathon are literally filled halfway. As are most marathons — by design. That is not a complaint about the volunteers. It is the operational reality every runner needs to know before they arrive at the start line. Full cups spill — vital XACT, Nuun, or Gatorade lost to the pavement; critical water gone before it reaches the runner who needs it to wash down a gel or cool down in the heat. So the rationale behind a half cup is sound.
What is not sound is the assumption — shared by the race and the runner alike — that one half-filled cup per station is enough.
For 2026, the race upgraded its electrolyte product to XACT Nutrition “Citrus Bang” — 500mg sodium per tablet dissolved in 500ml water, or approximately 1,000mg/L. More sodium-dense than sweat. More concentrated than Gatorade Endurance. More concentrated than any drink used at Boston, Chicago, or New York. The product upgrade is significant. The cup fill is the limiting variable.
The product upgrade gave with one hand. The cup fill — half a 6 oz cup — constrains what the hand delivers.
Manitoba Marathon: How much XACT most runners may need to consume
The fluid picture is solvable. A bigger cup — two 300ml cups, each half filled — at 16 stations delivers 4.8L of fluid: enough for 5 and 6-hour runners to finish within the planning threshold. More stations would help. So would knowing how much to drink per station — based on the number of stations on the course, your own personal sweat rate, the amount of fluid in the cup, and the amount of sodium in that same cup. Research suggests the optimal finish-line hydration target is a range of 1.0–1.5% body mass loss: enough dehydration to avoid overhydration risks while staying well below the performance threshold.
Here is what each runner may need to consume at Manitoba's 16 stations to land in that optimal zone:
Manitoba Marathon 2026 — optimal fluid and sodium by finish time
Assumptions: 85kg runner, 1L/hr sweat rate, 700mg/L sweat sodium, 16 stations, 90ml confirmed cup fill (6 oz cup filled halfway), XACT Nutrition 1,000mg/L. Target: 1.0–1.5% body mass loss at finish. Values above 100% sodium replaced reflect generous replacement within the range of individual sweat sodium variability (approximately 400–1,000mg/L). Excess sodium at these volumes poses no physiological risk for healthy runners.
Table 8 — Manitoba Marathon: How much XACT most runners may need to consume
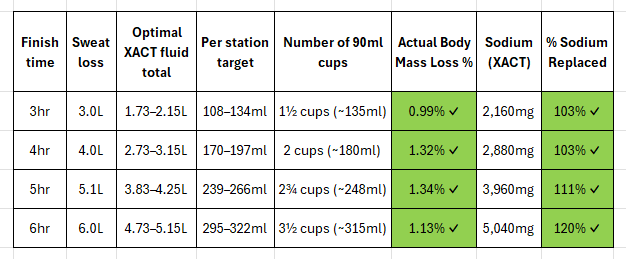
Every runner at optimal consumption replaces more sodium than they lose. Every row. Every finish time. Above 86%.
A note on the 1.0–1.5% actual body mass loss target: this is a hypothesis, not a law. The medical literature on optimal body mass loss during endurance events is evolving, not settled. What the research consistently supports is the direction of travel: the 2% threshold is associated with measurable performance decline; drinking to replace 100% of losses risks overhydration and hyponatremia; and modest, controlled dehydration — somewhere between 1% and 2% — appears to be where performance is best sustained for most recreational runners in most conditions.
The 1.0–1.5% window used in this table is a working planning target drawn from that literature. It is a reasonable hypothesis to train and race toward — not a clinical prescription, and not a number that applies equally to every runner in every condition. Individual sweat rates, body composition, fitness level, heat, humidity, and race pace all affect where any given runner’s optimal zone actually sits. This table is a starting point. The knowledge to refine it lives in your own training data — and in a bathroom scale used before and after a long run to confirm your rate of body mass loss in varying weather conditions.
On sodium, the 2026 Manitoba Marathon — if XACT is mixed at the published concentration of one tablet per 500ml — is now the best-provisioned race in this analysis on a per-litre basis. Better than Boston. Better than Chicago. Better than New York. The same station count as last year — and the year before that, going back at least to 1998. A significantly better drink than last year.
The race quietly made the most important hydration decision it could make. Nobody published the numbers. Now someone has.
Note: XACT “Citrus Bang” concentration confirmed at manufacturer specification — one 4.5g tablet dissolved in 500ml water — by Manitoba Marathon race management on May 26, 2026. Race operations pre-portion tablets in advance to ensure consistency.
On May 26-28, 2026 — four weeks before race day — Manitoba Marathon race management confirmed the following by email: 16 stations on the full marathon course, including a community-run station at km 40 and the official station at km 41; XACT Nutrition “Citrus Bang” electrolyte tablets mixed according to manufacturer specifications; electrolytes available at every aid station; stations remain operational until the sweep vehicle passes. Cup size is 6 oz (approximately 180ml), with volunteers instructed to fill cups approximately halfway — roughly 90ml of fluid per cup. The analysis above uses 90ml per cup as the confirmed planning assumption.
Are there things that the Manitoba Marathon could do better? Certainly. Are there things that I could do better? Absolutely. But in my experience, Manitoba keeps the covenant.
The station count has held for at least 28 years. For 2026, the drink finally caught up. That is the whole story.
Thirty years. The language now exists. The knowledge now exists. The arithmetic now exists. The body is still sending the same signal.
The Back of the Pack Is the Safety Test
Through the 1990s and into the early 2000s, sports medicine was advising runners to stay ahead of thirst — drink early, drink often, drink either standard Gatorade or water whether you felt like it or not. Many runners who followed that advice developed Exercise Associated Hyponatremia. The sodium in both standard Gatorade and plain water was too low to keep pace with what sweat was removing. Drinking large volumes of either simply diluted what remained.
It only just dawned on me, sitting here writing this piece, that my own stubborn one-cup habit had accidentally kept me on the right side of that line.
I never went past one cup of anything at any station across all my marathon years. When I was faster, that restraint worked in my favour — less time on course, less total sweat loss, and one cup per station coming reasonably close to matching what I was losing. I never ran into hyponatremia. I never overcorrected. The accidental tactic held.
But pace is not permanent. As I grew older and slower, more time on course meant more total sweat loss. The same one cup that once roughly balanced the equation began falling further and further behind.
The tactic that protected a 3:30 runner was quietly failing a 5:06 one. Prague was the first time the gap was large enough to show up on a bathroom scale.
World Athletics grants Elite Label status based on standards: course certification, timing, elite fields, anti-doping, prize structures, operational requirements, and organizational quality. Elite Label status is also sold to host cities and municipalities as a tourism and marketing asset — a signal of international prestige, broadcast reach, and economic impact.
The incentive structure points toward spectacle. It does not point toward the 4, 5, or 6-hour runner at km 33.5.
That label may mean a great deal for the front of the race.
What it does not make transparent to recreational runners is how well the race serves the back of the field: the runners finishing in four, five, six, or seven hours.
The elite runner finishes before the day reaches its warmest point.
The five-hour runner lives in a different race.
The elite runner passes through pristine stations.
The five-hour runner discovers whether the refill plan works.
The elite runner runs before the volunteers are tired.
The five-hour runner finds out whether the tables are still up.
The elite runner tests the race’s speed.
The back of the pack tests the race’s system.
By the time Group K arrived at km 33.5, the race had been underway for hours. The visible spectacle had long since moved on. The winners were finished. The broadcast story was complete. But thousands of ordinary runners were still out there — runners carrying the greatest cumulative heat load, fluid deficit, sodium deficit, and time on feet.
The first four-hour finisher placed 3,745th, meaning more than 5,300 official finishers still came after the four-hour mark. The first five-hour finisher placed 7,473rd — with approximately 1,600 runners still behind them. The first six-hour finisher placed 8,789th — with approximately 270 runners still on course.
The infrastructure choices that matter most at km 33.5 are not the ones that earned the World Athletics Elite Label. They are the ones that determine whether a back-of-pack runner with five hours of cumulative fluid and sodium debt finds a fully stocked electrolyte station, a clearly differentiated cup, and supply that has not been packed up because the broadcast story is finished.
That is not the least important part of the race.
It is the part where safety matters most.
This is not only a Prague problem. It is a structural problem in prestige marathon management.
Prestige points forward. Risk accumulates backward.
The system should be designed accordingly.
Every participant in a World Athletics Label marathon must be treated as an athlete, whether they finish in the top 100 or the bottom 1,000.
That is the standard. Or it should be.
What Right Looks Like
White cups for water. Green cups for Gatorade.
The single cheapest fix in this letter.
Here is what I would do differently — not as a complaint, but as a proposal. We have the tools to design a marathon that serves its entire field, not just its fastest tenth.
None of what follows absolves the runner. We have to train for the time we are actually fit to run. We have to read the published aid plan and think it through. We have to carry supplemental sodium and carbs if our math says we need it. We have to adjust on race morning when the weather is not what we expected.
I did some of these things at Prague. I did others poorly.
The 135 mg sodium I left on the course at two gel stations is on me. The fact that very likely, over the past 42 years, I have only ever drunk one cup of either electrolyte replacement fluid or plain water at each station instead of two — is on me. The training that supported a five-hour finish rather than a four-hour finish is on me. A well-designed race does not remove the need for personal accountability. It makes responsible planning possible. The current information gap makes responsible planning far harder than it needs to be for the majority of the field.
Electrolyte drink should be available at sufficient station density that a five or six hour runner can realistically meet both fluid and partial sodium targets without heroic cup consumption. Whether that means every station or close to it depends on the drink concentration the race chooses to serve. The math is the test.
Station density should be based on what a tired runner can actually drink from a half-filled cup, not what a spreadsheet says is theoretically available in litres.
Published numbers. Cup size. Expected pour volume. Sodium per litre. Carbohydrate per litre. Drink mix protocol. Electrolyte station locations. Water-only station locations. Salt availability. Late-course supply policy. These are not trade secrets. They are the raw materials of a runner’s survival plan.
Personalized pre-race hydration estimates should not be impossible. Not a generic FAQ buried on the race website — a calculated, individualized estimate delivered by email to each registered runner two to three weeks before race day, based on body mass, age, sex, and declared expected finish time. Something like: “You are likely to sweat approximately X litres over your expected race duration. Practical fluid replacement target is Y. Here is how many stations carry electrolyte drink, at what kilometre markers, with what sodium concentration. Here is what you should consider carrying for sodium beyond what the race provides. Adjust your intake on race day based on the weather.”
Runner Base Knowledge. If a driver’s licence requires proof that I understand the rules of the road before I am allowed onto the highway, a marathon registration could reasonably ask whether I understand the basic physiology of what I am about to do — how much fluid I expect to lose over my projected finish time, and how the course is designed to help me replace it.
The driving instructor is protecting everyone on the road, including the wanna be driver. The marathon director should be protecting the runner from running themselves into the ground.
Literally.
Overhead station signage. WATER. GATORADE. FRUIT. SALT. SUGAR. Big enough for the incoming runner to see before entering the congestion. Differently coloured cups for different fluids — and different in a way that is visible at pace. White for water. Green for Gatorade. Not black-and-white for water and white-and-black for Gatorade.
Late-course supply planning based on when runners actually arrive, not just where stations sit on the map. A station at km 33.5 serves a very different physiological population at noon than it does at 8:30.
Operationally distinct water supplies. If water is supplied from a tanker, organizers should be clear whether it is potable drinking water or cooling water. Those are not interchangeable categories. If drinking water is also expected to serve as cooling water, station supply calculations must account for that.
Cobblestone surfaces. Historic street networks are beautiful. In my personal experience as a runner, they are also a concentration-demanding surface when legs are failing after four or more hours. This is an observational judgment, not a claim backed by injury-rate data — but it is worth factoring into course design. Use them early for atmosphere. Use smoother surfaces later when fatigue is highest.
Shade mapping as part of course design. Satellite and canopy data can identify shaded corridors in a city. A course can be routed to maximize tree cover during the hours when back-of-field runners will be present.
Separate the problem. The simplest fix may be the one no marathon director wants to hear: stop trying to serve a precisely mixed electrolyte drink from a moving aid station. Provide plain water at every station, publish the cup size, and let runners who have done the math carry their own sodium. A 250 mg electrolyte gel consumed with 300 ml of water produces a known concentration from a known dose. The race cannot accidentally dilute it. The volunteer cannot misidentify it. The runner cannot grab the wrong cup. The experiment is controlled because the variables are separated: the race provides the solvent, the runner provides the solute.
This is not a counsel of despair for back-of-pack runners. It is a redistribution of responsibility toward the party that can exercise precision. A race can reliably deliver water at consistent volumes from clearly marked cups. It cannot reliably deliver a sodium concentration that varies with mixing protocol, volunteer fatigue, temperature, and late-race supply management. A runner who has done their sweat math can carry exactly the sodium they need, add it to any cup of water on any course, and know exactly what they consumed. That is more than Prague or any marathon could ever promise.
The self-supply argument has a limit: it only works for runners who know they need to bring sodium. Most runners in Corral K do not. A 4-hour marathoner who grabs a single cup of Gatorade Endurance at every aid station at Boston will likely finish within safe physiological bounds — the drink is concentrated enough to deliver meaningful sodium at a single realistic cup, even without any planning. A 4-hour marathoner who does the same at Berlin — one cup of Maurten per station — will likely end up in a medical tent, because Maurten’s on-course drink provides almost no sodium at any volume. The uninformed runner needs the drink to protect them. The informed runner can supplement whatever the course provides.
The actual design goal is a course that covers both. Provide a drink concentrated enough to matter for the runner who grabs one cup and keeps moving. Tell that runner what is in it. Let runners who want more bring more. That combination protects the field from the front runner finishing in two and a half hours to the back-of-pack runner still out there at hour five — in a way that neither Berlin’s self-supply model nor Prague’s dilute-drink-plus-alternating-stations model achieves.
A post-finish recovery chute. Not a banana half a kilometre away. A flow-through system with water, electrolyte replacement, fruit, carbohydrate replacement, and medical observation before runners exit the controlled finish area.
The data exists to build this race. What is missing is the decision to ask what the runner at km 35 actually needs, and to treat that question as seriously as the question of what the elite runner at km 35 needs.
Prague did not fail because it served the wrong drink. It failed the back of the field — the runners still out there at hour five and six — because it presented an electrolyte system that appeared precise enough to plan around, while withholding the operational details needed to make that precision real, and while those runners were still out there, still sweating, and still guessing.
The Covenant
An organization can do many things well and still miss the thing directly in front of it.
It can stage a beautiful race and still underserve the runners who spend the longest time on the course. It can attract elite athletes and still fail to design its aid stations around the people most dependent on them. It can meet World Athletics standards for elite field management and still fail to meet physiological safety margins for the back of the pack. It can provide a magnificent finish screen and still make a five-hour runner walk half a kilometre for a banana.
That gap is where the runners fall.
The elites are housed, transported, and paid prize money. They are a cost line in the spreadsheet.
The non-elites are the entire business model.
And the most important non-elites are not the international tourists like me, making a once-in-a-decade trip to Prague. They are the Czech runners from Brno, Ostrava, Plzeň, and every running club that feeds this race year after year. They are the ones who will decide whether to register again. They are the ones who will tell twenty people exactly what they found, or did not find, at km 33.5.
The tables in this piece show a runner crossing the 2% threshold at approximately km 30 and never recovering. From that point forward, the legs were running against a deficit the course created before the starting gun fired. The 5:06 finish was not a fitness failure. The training supported a faster race. The deficit was operational. It was built into the course architecture long before the race began.
Better hydration infrastructure almost certainly would have given me better physiological margin in the final third. By how much is impossible to say without real race data — five minutes, fifteen, or more. What the tables show is that the physiological deficit was real, it was building from km 1, and it was entirely preventable.
Now multiply that across 11,800 runners.
Not all of them were dehydrated to the same degree. Not all of them were medium sweaters at 85kg. But a meaningful fraction of the field was running the same Table 1 race — one cup, wrong stations, wrong drink, wrong concentration — and paying the same price in the back half. If proper hydration infrastructure recovers even fifteen minutes from the median back-of-pack finisher, the aggregate time returned to the field is staggering. More finishes under six hours. Fewer medical interventions. More runners crossing the line feeling like runners instead of survivors.
And beyond the time: more people who come back next year. More people who tell someone the race was worth it. More people who lace up again because the experience did not break them.
A well-hydrated field is a faster field. A faster field is a healthier field. A healthier field comes back.
In my experience, my hometown marathon, the Manitoba Marathon, keeps the covenant.
You give them your Sunday morning and your entry fee. They give you shade, neighbours, electrolytic fluids and water at every aid station, a world class finish-line and recovery, and the dignity of being treated as the reason the race exists.
That is all it takes.
Shade. A sign. A cup that clearly tells you what is in it. Electrolytes where runners need them. A banana before half a kilometre of walking — after you have already run 42.195 km. And the numbers a runner needs to plan the race he is actually about to run.
You do not need a World Athletics Elite Label to get that right.
You just need to remember why you started doing this thing in the first place.
And you need to remember who the race is for.
Regards,
Luke Kandia
Luke Kandia is an investigative writer and researcher based in Winnipeg, Manitoba, and a recreational runner. He has formally submitted a runner safety complaint to RunCzech regarding the Vodafone Prague Marathon 2026; RunCzech replied substantively on May 10, but a detailed follow-up sent on May 11 had received no response as of publication. He has also attempted to bring the same concerns to the attention of World Athletics; no response from World Athletics has been received as of publication. Runners who experienced similar conditions on May 3 are invited to share their observations in the comments.
If you are a marathon director and you are reading this: the data to fix these problems exists. The will to use it is the only missing variable.
This article is a personal account and operational analysis. It is not medical advice. The physiological claims made throughout the body of this piece, including fluid targets, sodium estimates, and references to hyponatremia and dehydration risk, reflect the author’s interpretation of published research and personal observational data, not clinical guidance. Individual hydration and sodium needs vary widely. Runners considering changes to their race-day fluid and electrolyte strategy should consult with a sports medicine professional, registered dietitian, or qualified coach, and should test any new strategy in training before applying it on race day.
Postscript: Two articles, three dates, one story
On May 2, 2026, the day before the race, RunCzech published a pre-race safety guide. It contained five tips from their medical team. Tip 5 advised runners to drink proactively at every station, adding: “It is advisable to alternate water with an isotonic drink, which replenishes fluids, minerals and energy.” Their medics also noted that “just a few sips will not slow you down significantly.”
That is the half cup problem, written by the race organiser, published the day before the race.
A few sips.
Not two cups. Not the arithmetic. Not a sodium target. Not a milligram. The word “minerals” appeared once in five tips. That was the entirety of the sodium guidance available to 11,800 runners standing on the start line the following morning.
The same article confirmed that RunCzech had deployed 34 medical points along the route — one for approximately every kilometre of racing. There were 16 aid station encounters on the course. Eight of them had electrolytes.
The race was prepared to treat the problem at more than twice the density it was prepared to prevent it.
On May 3, 2026, they ran the race described in this piece.
On May 13, 2026, RunCzech published a post-race medical review. Their Running Doctors reported conditions reaching 30°C under direct sun. The team confirmed they had monitored runners specifically for dilutional hyponatremia, the condition where excess plain water at the expense of sodium can become life-threatening. Their post-race recovery advice was to drink water with approximately half a teaspoon of salt per litre, because plain water consumed without sodium replacement is largely excreted without physiological benefit.
The knowledge was there on May 2. The confirmation was there on May 13.
On May 3, the cups were black and white, half the station encounters had no electrolytes, and the sodium concentration, pour volume, and mixing protocol were never published.
One more detail.
RunCzech’s primary hydration sponsor is Mattoni — a plain mineral water company whose branding appeared on the water cups throughout the course. The same May 13 post-race medical article concluded with a promotional statement from Mattoni’s Senior Brand Manager describing the product as ideal for “quality hydration.” The next RunCzech event, the Mattoni Karlovy Vary Half Marathon, features Mattoni as title partner, with hydration described as a key theme.
The sponsorship and the clinical reality were published on the same page, in the same article, ten days after the race.
RunCzech’s own doctors had already stated that plain water without sodium replacement is largely excreted without benefit. Their own pre-race guide advised runners to alternate water with isotonic drink. Their own course provided isotonic drink at eight of sixteen station encounters, in cups that looked nearly identical to the water cups, without publishing the sodium concentration, the pour volume, the mixing protocol — or why any of that mattered.
The problem was not that RunCzech lacked the knowledge. It was that what they knew did not make it into the cup.
Sources and Notes
Primary sources
RunCzech / Vodafone Prague Marathon 2026
RunCzech. Safely to the finish: The Vodafone Prague Marathon looks after runners’ health at every kilometre. May 2, 2026. https://www.runczech.com/en/useful/for-the-media/news/safely-to-the-finish-the-vodafone-prague-marathon-looks-after-runners-health-at-every-kilometre
RunCzech. Health first! Running doctors helped directly on the course. May 13, 2026. https://www.runczech.com/en/useful/for-the-media/news/health-first-running-doctors-helped-directly-on-the-course
Vodafone Prague Marathon 2026 official event page and racer FAQ. runczech.com. Accessed May 2026.
Vodafone Prague Marathon 2026 official results database. RunCzech. Accessed May 2026.
RunCzech post-race email to registered participants, May 8, 2026. Private communication to author.
RunCzech email reply to author regarding race operations. Private communication to author.
Manitoba Marathon
Manitoba Marathon race management. Email correspondence with author, May 26, 2026. Confirming station count, XACT product, mixing specification, and cup fill volume.
Manitoba Marathon 2026 course map and participant handbook. manitobamarathon.mb.ca. Accessed May 2026.
Winnipeg Free Press. Manitoba Marathon course map. June 20, 1998, p. 66.
Hamiota Echo. Manitoba Marathon race report. July 4, 1995, p. 3.
Product specifications
XACT Nutrition. Electrolytes Hydration Tabs — Citrus Bang. xactnutrition.com. Accessed May 2026.
Nuun Sport. Electrolyte tablets product page. nuunlife.ca. Accessed May 2026.
Gatorade. Endurance Formula product specification. gatorade.com. Accessed May 2026.
Maurten. General Product FAQ. maurten.com/faq/general-product. Accessed May 2026.
Author data
Garmin Connect activity record, Vodafone Prague Marathon, May 3, 2026. Personal data.
Garmin Connect weigh-in records, 2025–2026. Personal data.
Precision Hydration. Personalized fuel and hydration plan. Generated at precisionhydration.com using author’s personal data. Accessed May 2026.
© Lucas Kandia, 2026. All rights reserved.
Scientific literature
Bryson Carrier, Amanda C Melvin, Jacob R Outwin, Marni G Wasserman, Adam P Audet, Katherine C Soldes, Kenneth M Kozloff , Adam S Lepley. Evaluation of Exertional Sweat Loss Estimates in Wearable Technology. Sports Health. 2025 Nov 30. doi:10.1177/19417381251388642. PMID: 41320899. (Garmin mean absolute percentage error approximately 33% overall; approximately 39% in male runners; individual variation ranged from several hundred millilitres under to several hundred millilitres over actual measured loss. Conclusion: wearable sweat estimates suitable for trend tracking but not precise enough to replace weigh-ins when accuracy matters.)
Sawka MN, Burke LM, Eichner ER, Maughan RJ, Montain SJ, Stachenfeld NS. American College of Sports Medicine position stand. Exercise and fluid replacement. Medicine & Science in Sports & Exercise. 2007.
Goulet EDF. Effect of exercise-induced dehydration on endurance performance: evaluating the impact of exercise protocols on outcomes using a meta-analytic procedure. British Journal of Sports Medicine. 2011.
Hew-Butler T, Rosner MH, Fowkes Godek S, Dugas JP, Hoffman MD, Lewis DP, Maughan RJ, Miller KC, Montain SJ, Rehrer NJ, Roberts WO, Rogers IR, Siegel AJ, Stuempfle KJ, Winger JM, Verbalis JG. Statement of the Third International Exercise Associated Hyponatremia Consensus Development Conference, Carlsbad, California, 2015. Clinical Journal of Sport Medicine. 2015.
Hew-Butler T, Loi V, Pani A, Rosner MH. Exercise Associated Hyponatremia: 2017 Update. Frontiers in Medicine. 2017.
Almond CSD, Shin AY, Fortescue EB, Mannix RC, Wypij D, Binstadt BA, Duncan CN, Olson DP, Salerno AE, Newburger JW, Greenes DS. Hyponatremia among Runners in the Boston Marathon. New England Journal of Medicine. 2005. (13 percent of a sampled field of finishers met the clinical threshold for hyponatremia; weight gain during the race, longer race time, and BMI extremes were associated with hyponatremia on multivariate analysis; fluid composition — water versus sports drink — was not independently associated with hyponatremia; commercial sports drinks were noted as too dilute in sodium to offset risk from large fluid volumes.)
Baker LB. Sweating Rate and Sweat Sodium Concentration in Athletes: A Review of Methodology and Intra/Interindividual Variability. Sports Medicine. 2017.
Featherstone M. Nutrition tips for the Abbott World Marathon Majors. Featherstone Nutrition. May 15, 2024. https://www.featherstonenutrition.com/nutrition-tips-for-the-world-marathon-majors/
Glad I am not a runner, cause I would have to be a scientist also.